
On the face of it, it seems self-evident that a New Zealand libertarian party would be a staunch supporter of cannabis law reform. There’s nothing less libertarian than the government putting people in cages for using a medicine they don’t approve of, and there’s nowhere in the world with a greater appetite for a repeal of cannabis prohibition.
The New Zealand ACT Party claims to be a libertarian party. They have wrapped themselves in the libertarian yellow and their website boldly states “We believe the current role of government is far too large and should be limited on a principled basis.”
Sounds good, as probably 75% of New Zealand agrees that the New Zealand Government’s decades-long war on medicinal cannabis users has been a governmental overreach and should be limited.
The ACT Party Crime and Justice page even goes as far as to state, at the top: “We’re striving for a progressive, vibrant New Zealand that encourages individual choice, responsibility and excellence.”
From all this rhetoric you’d think a repeal of cannabis prohibition would be front and centre, but it’s not even mentioned. Instead the entire Crime and Justice section is just a lengthy diatribe about how burglary is the greatest evil facing our nation and ought to be punished severely.
The inability of the ACT Party to make good on their rhetoric about compassion and freedom by supporting a repeal of New Zealand’s cannabis laws – despite their unprecedented degree of leverage on the current Government – marks that party, and David Seymour, as a pack of weaklings.
What takes the ACT Party’s behaviour from disappointing to pathetic is the fact that it has already been well established that a repeal of our cannabis laws would save the taxpayer $400,000,000 per year.
So changing our cannabis laws, and making good on all the lofty rhetoric about compassion and freedom and fulfilling New Zealand’s destiny as a forward-thinking nation, would be a simple matter of negotiating with the current National Government $400,000,000 worth of tax cuts that would be paid for with the savings from cannabis prohibition.
It isn’t clear why Seymour has yet to kick the ball into this wide open goal.
Probably because he is a coward, but it’s unlikely that a man could possibly be so craven. Imagine being so gutless, so lily-livered, so chickenshit, that a 76-year old former leader of your party was saying what needed to be said six years ago, and you still can’t find the stomach to walk the same trail blazed by this geriatric.
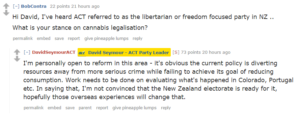
A more charitable explanation though, going by his wittering about the need to do work on evaluating what’s happening overseas, is that Seymour is just in the same twenty-year time warp as most of the rest of the country.
It was pointed out in a previous Dan McGlashan column that supporting the ACT Party has a very strong negative correlation with being born in New Zealand (-0.74). Has the ACT Party sold its soul to corporate globalist interests so that Seymour could be a National party puppet?
Considering that there are significant correlations between voting ACT and both having a professional occupation, or with working in financial and insurance services, it’s unlikely that ACT voters or supporters have much in common with cannabis users at all, much less using cannabis themselves.
If those are the circles Seymour moves in, perhaps this is why Seymour has failed to observe the immense appetite for a change to our ridiculous laws.
So maybe he needs to climb down out of the ivory tower and get a clue.
Coming out in support of cannabis law reform would lend credence to the idea that ACT might really be a libertarian party, instead of what most Kiwis suspect them to be – paid whores of big corporate interests.
The question is whether Seymour has the courage to stand up to a Catholic prohibitionist National Party leader, or whether he’d rather scurry away and prepare himself for the aftermath of the likely National loss later this year.
The most sure thing of all is that if ACT does not make an appeal to libertarian New Zealanders by updating their cannabis policy, they have little hope of winning more than one seat in this year’s election.